
The relationship of the basilar artery bifurcation and dorsum sel lae
Umístění bifurkace bazilární tepny ve vztahu k dorsu sellae
Cíle:
Cílem studie bylo zhodnotit postavení bifurkace bazilární tepny (BAB) ve vztahu k dorsu sellae (DS) na základě CT snímků hlavy. BAB většinou tvoří dva segmenty P1 zadních mozkových arterií na úrovni fossa interpeduncularis v těsné blízkosti DS. Tento typ rozdvojení se nazývá bifurkace. V této oblasti může vznikat řada patologií, vč. aneuryzmat BAB, která představují asi 5– 8 % všech intrakraniálních aneuryzmat. V literatuře se uvádí, že umístění aneuryzmatu ve vztahu k DS hraje důležitou roli při plánování chirurgické léčby aneuryzmat v oblasti BAB.
Soubor a metodika:
Do studie bylo zařazeno 100 CT angiografických snímků pořízených u 54 žen and 46 mužů ve věku 18– 88 let (průměrný věk 52,49 let). K analýze byly použity multiplanární rekonstrukce. V koronárním řezu byla analyzována pozice BAB ve vztahu ke střední sagitální rovině (MP) a nejnižšímu bodu DS (LDSP) v transverzální rovině (TP). V sagitálním řezu byla zjišťována vzdálenost mezi BAB a DS.
Výsledky:
U sledovaných pacientů (n = 100) byla BAB v 57 % případů umístěna napravo od MP, zatímco ve 41 % případů se nacházela nalevo a ve 2 % případů ve střední rovině. U 47 % pacientů byla BAB umístěna nad LDSP (TP) a u 53 % pacientů pod ním. Umístění v TP nebylo zjištěno ani v jednom případě. Průměrná vzdálenost mezi BAB a MP byla 0,35 mm; SD 1,91 mm, a průměrná vzdálenost mezi BAB BBT a TP byla 1,01 mm; SD 4,47 mm. Průměrná vzdálenost mezi BAB a DS byla 9,34 mm; SD 2,61 mm.
Závěry:
Studie neodhalila statistické významné rozdíly v umístění BAB v závislosti na pohlaví. Vysoce významný rozdíl byl však zjištěn u osob starších než 45 let, u nichž byla BAB umístěna výše nad TP (ve vztahu k DS).
Klíčová slova:
bifurkace bazilární tepny – hrot bazilární tepny – aneuryzma bazilární tepny – dorsum sellae – výpočetní tomografie
Autoři deklarují, že v souvislosti s předmětem studie nemají žádné komerční zájmy.
Redakční rada potvrzuje, že rukopis práce splnil ICMJE kritéria pro publikace zasílané do biomedicínských časopisů.
Authors:
W. Ilków 1; M. Waligóra 2; M. Kunc 3; M. Kucharzewski 4
Authors place of work:
Department of Neurosurgery, University Teaching Hospital in Opole, Poland
1; Department of Medical Imaging, VITAL MEDIC, Kluczbork, Poland
2; Helimed Imaging Center, Opole, Poland
3; School of Medicine with the Division of Dentistry in Zabrze, Department and Division of Descriptive and Topographic Anatomy, Medical University of Silesia in Katowice, Zabrze Rokitnica, Poland
4
Published in the journal:
Cesk Slov Neurol N 2018; 81(5): 576-581
Category:
Původní práce
doi:
https://doi.org/10.14735/amcsnn2018576
Summary
Aims:
The aim of the study was to assess the position of the terminal basilar artery bifurcation (BAB) in relation to the dorsum sellae (DS) based on CT scans of the head. The BAB is, in most cases, formed by two P1 segments of the posterior cerebral arteries at the level of the interpeduncular fossa, in close proximity to the DS. This type of division is called bifurcation. Numerous pathologies may develop in this region, including BAB aneurysms, which account for 5– 8% of all intracranial aneurysms. The literature states that the position of an aneurysm in relation to the DS plays a significant role in planning surgical strategies for BAB aneurysms.
Patients and methods:
The study involved 100 CTA scans of 54 women and 46 men in a range of 18– 88 years of age (mean age 52.49 years). Multiplanar reconstructions were used. The position of the BAB in relation to the sagittal midline plane (MP) and the lowest DS point (LDSP) in the transverse plane (TP) was analysed in the coronal section. The distance between the BAB and the DS was measured in the sagittal section.
Results:
In the studied patients (n = 100), the BAB was located on the right of the MP in 57% of the cases, on the left of the MP in 41% of the cases and in the midline or median position in 2% of the cases. The BAB was located above the LDSP (TP) in 47% of the cases, and below it in 53% of the cases. There were no cases in which the BAB was located in the TP. The average distance between the BAB and the MP was 0.35 mm; SD 1.91 mm, and the average distance between the BAB and the TP was 1.01 mm; SD 4.47 mm. Moreover, the average distance between the BAB and the DS was 9.34 mm; SD 2.61 mm.
Conclusions:
The study revealed no statistically significant differences in the BAB position depending on gender. However, a highly significant difference and higher location of the BAB in relation to the TP (in relation to the DS) was observed in persons above 45 years of age.
Key words:
basilar artery bifurcation – basilar artery tip – basilar artery aneurysm – dorsum sellae – computed tomography
Chinese summary - 摘要
基底动脉分叉与背鞍的关系
目的:
该研究的目的是根据头部的CT扫描评估末端基底动脉分叉(BAB)相对于鞍背(DS)的位置。 在大多数情况下,BAB由位于椎间窝水平的两个大脑后动脉的P1段形成,紧邻DS。 这种划分称为分叉。 该区域可能出现许多病变,包括BAB动脉瘤,占所有颅内动脉瘤的5-8%。 文献指出动脉瘤相对于DS的位置在规划BAB动脉瘤的手术策略中起重要作用。
患者和方法:
该研究涉及对54名女性和46名男性进行100次CTA扫描,范围为18-88岁(平均年龄52.49岁)。 使用多平面重建。 在冠状切面中分析BAB相对于矢状中线平面(MP)的位置和横向平面(TP)中的最低DS点(LDSP)。 在矢状切面测量BAB和DS之间的距离。
结果:
在研究的患者(n = 100)中,57%的病例BAB位于MP的右侧,41%的病例位于MP的左侧,2%的病例位于中线或中位。BAB在47%的病例中位于LDSP(TP)之上,在53%的病例中位于其之下。 没有BAB位于TP的情况。 BAB和MP之间的平均距离为0.35 mm; 标准尺1.91毫米; BAB与TP之间的平均距离为1.01 mm; 和SD 4.47毫米。 此外,BAB和DS之间的平均距离为9.34毫米; SD 2.61毫米。
结论:
该研究显示,根据性别,BAB位置无统计学差异。 然而,在45岁以上的人群中观察到BAB相对于TP(相对于DS)的高度显著差异和更高的位置。
关键词:
基底动脉分叉 - 基底动脉尖 - 基底动脉瘤 - 背鞍 - 计算机断层扫描
Introduction
Basilar artery bifurcation (BAB) is in most cases formed by two P1 segments of the posterior cerebral arteries at the level of the interpeduncular fossa, in close proximity to the dorsum sellae (DS). This type of division is called bifurcation.
Below the bifurcation, the paired superior cerebellar arteries branch off of the basilar artery.
Together with two posterior cerebral arteries, they may co-form the BAB quadrifurcation, which is observed in 38% of the cases [1,2].
Numerous pathologies may develop in this region, including BAB aneurysms, which account for over 50% of vertebrobasilar aneurysms and 5– 8% of all intracranial aneurysms [3].
Due to the location of the BAB in proximity to vital anatomical structures, such as the brain stem, the internal carotid artery, the pituitary stalk and the oculomotor nerve, microsurgical treatment of BAB aneurysms still carries the risk of death at the level of almost 9– 10% [4– 8]; in the case of endovascular treatment, the risk is approximately 1.3– 2.7% [9,10]. Surgical conditions are additionally complicated by the fact that the arteries forming the BAB give off numerous and fragile perforators responsible for blood supply to the diencephalon and mesencephalon. Intraoperative damage to these may lead to death or severe defects [11].
In 1932, Herbert Axel Olivecrona was the first to operate on a patient with an aneurysm of the posterior circle of Willis. However, the pioneer of surgery on basilar artery aneurysms was Charles George Drake who, in the late 1950s, presented infratemporal access to the BAB by temporal lobe retraction [12]. This provides a lateral view at the BAB and the perforators. However, the risk of damaging the temporal lobe or insufficient inspection of the contralateral posterior cerebral artery, which are associated with this approach, prompted researchers to search for other routes of access [5]. In 1976, Gazi Yasargil proposed the anterolateral (pterional) approach through the Sylvian fissure, which makes the BAB accessible through a narrow window formed between the internal carotid artery and the oculomotor nerve. This does not necessitate temporal lobe retraction but still allows assessment of the initial segments of the posterior cerebral arteries. However, this approach is associated with a deep and narrow surgical field with a limited view into the posterior surface of the BAB [2,3].
Despite the development of endovascular methods of aneurysm treatment, which are also employed in the treatment of BAB aneurysms, surgery is still necessary when these techniques are ineffective or cannot be used [13,14].
Numerous authors believe that the position of an aneurysm in relation to the DS plays a decisive part in the surgery planning since, when located low, the DS may conceal the site of vascular clamping [15,16].
The aim of the study was to evaluate the position of the BAB in relation to the DS based on multiplanar reconstructions of CTA scans.
Patients and methods
The retrospective study involved 100 anonymised head scans from CTA of 54 women and 46 men in a range of 18– 88 years of age (mean age 52.49 years) diagnosed with headaches in 2012– 2016.
The scans were free of motion artefacts or foreign bodies, e. g. vascular clamps. The study excluded patients:
- after craniocerebral trauma;
- after a neurosurgical procedure (including endovascular) within the head;
- with a diagnosed intracranial tumour;
- with pathology within the vessels of the CNS.
The distance between the BAB and the sagittal midline plane (MP) as well as the transverse plane (TP) selected at the lowest DS point was determined using the bone window (W = 1500, L = 300) for CTA with multiplanar reconstruction. The distance between the BAB and the DS was measured in the sagittal section. The statistical analysis was conducted for the BAB position depending on gender and age (the analysed age groups were: group 1 – up to 45 years of age; group 2 – over 45 years of age).
Determination of the BAB
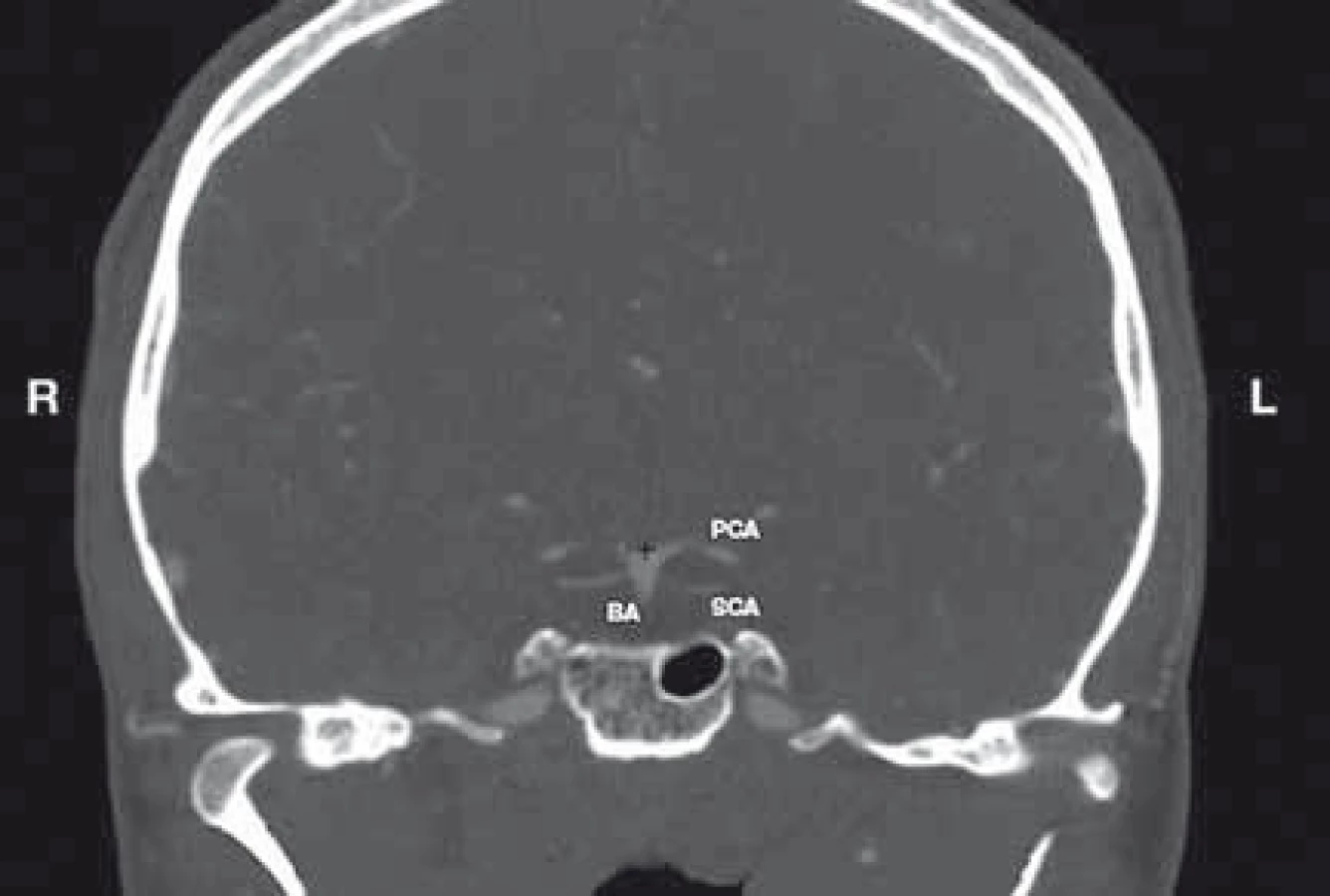
The BAB was determined in the coronal section of CTA at the site where both P1 segments of the posterior cerebral arteries originate. This point was marked on the screen using a marker (cross) (Fig. 1).
BA – basilar artery; BAB – basilar artery bifurcation; L – left; R – right; PCA – posterior cerebral artery; SCA – superior cerebellar artery
+ a marker
Obr. 1. Určení BAB. Koronární rekonstrukce CTA hlavy.
BA – bazilární arterie; BAB – bifurkace bazilární arterie; L – vlevo;
PCA – arteria cerebri posterior; R – vpravo; SCA – arteria cerebelli
superior
+ označení
Position of the BAB in relation to the DS
The coronal CTA scans were used to visualise the DS and to determine the MP and the lowest DS point (LDSP) within the TP. Subsequently, the BAB position was saved on the workstation screen with a marker (cross) and, using multiplanar reconstructions, its position was mapped in relation to the analysed planes (in relation to the DS).
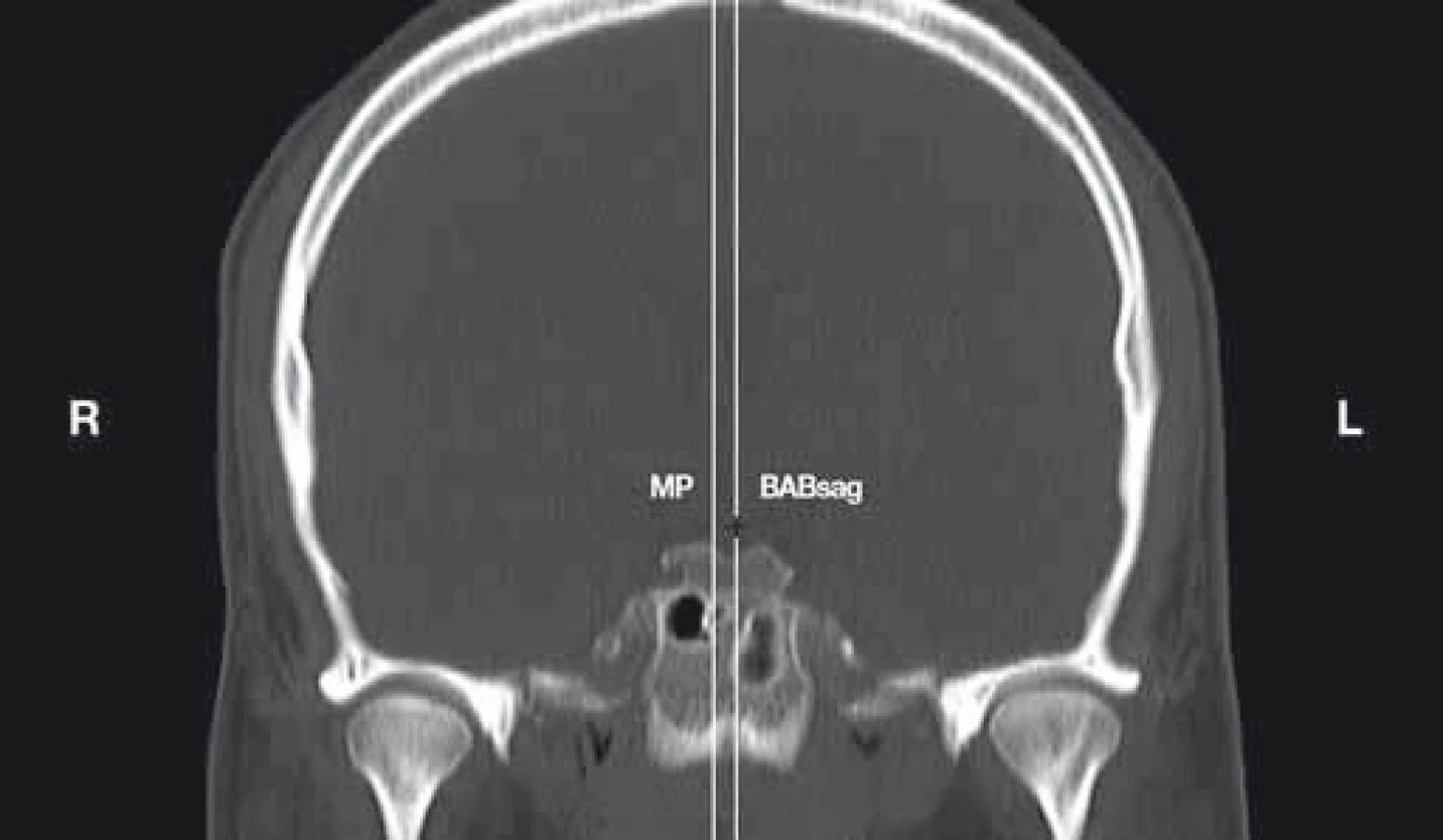
- A. In order to evaluate the position of the BAB in relation to the MP, the sagittal plane BABsag, parallel to the MP and encompassing the BAB, was selected. In the case of the BAB position on the right of the MP, negative values were assumed, whilst positive values were used when it was located on the left of the plane. In the case of the midline BAB location in the MP, the 0 value was assumed (Fig. 2).
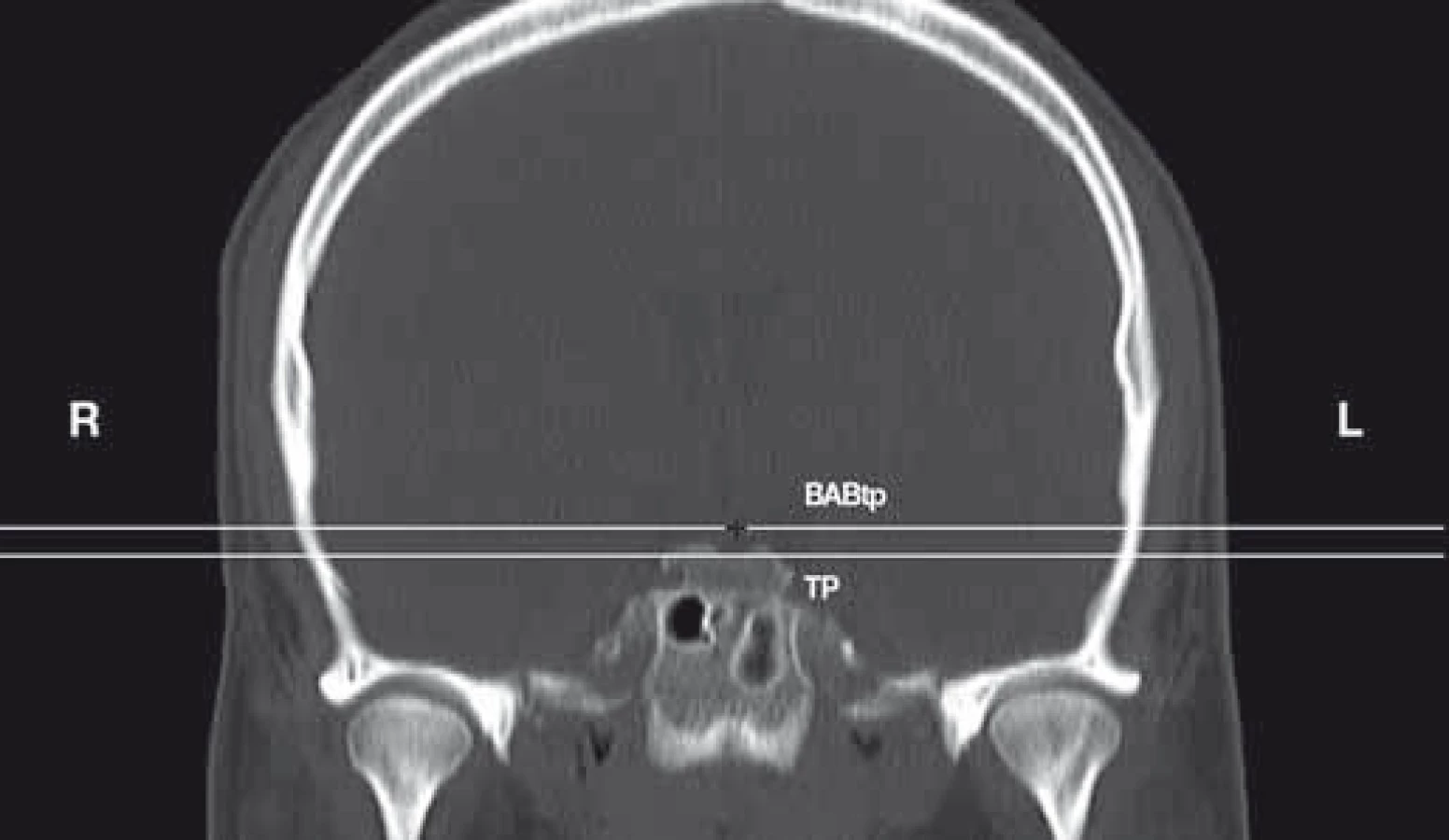
- B. In order to evaluate the position of the BAB in relation to the LDSP, the BABtp plane, parallel to the TP including the LDSP and encompassing the BAB, was selected. In the case of the BAB position above the LDSP (TP), positive values were assumed, whilst negative values were used when it was located below the plane. In the case of BAB location on the level of the LDSP (TP), the 0 value was assumed (Fig. 3).
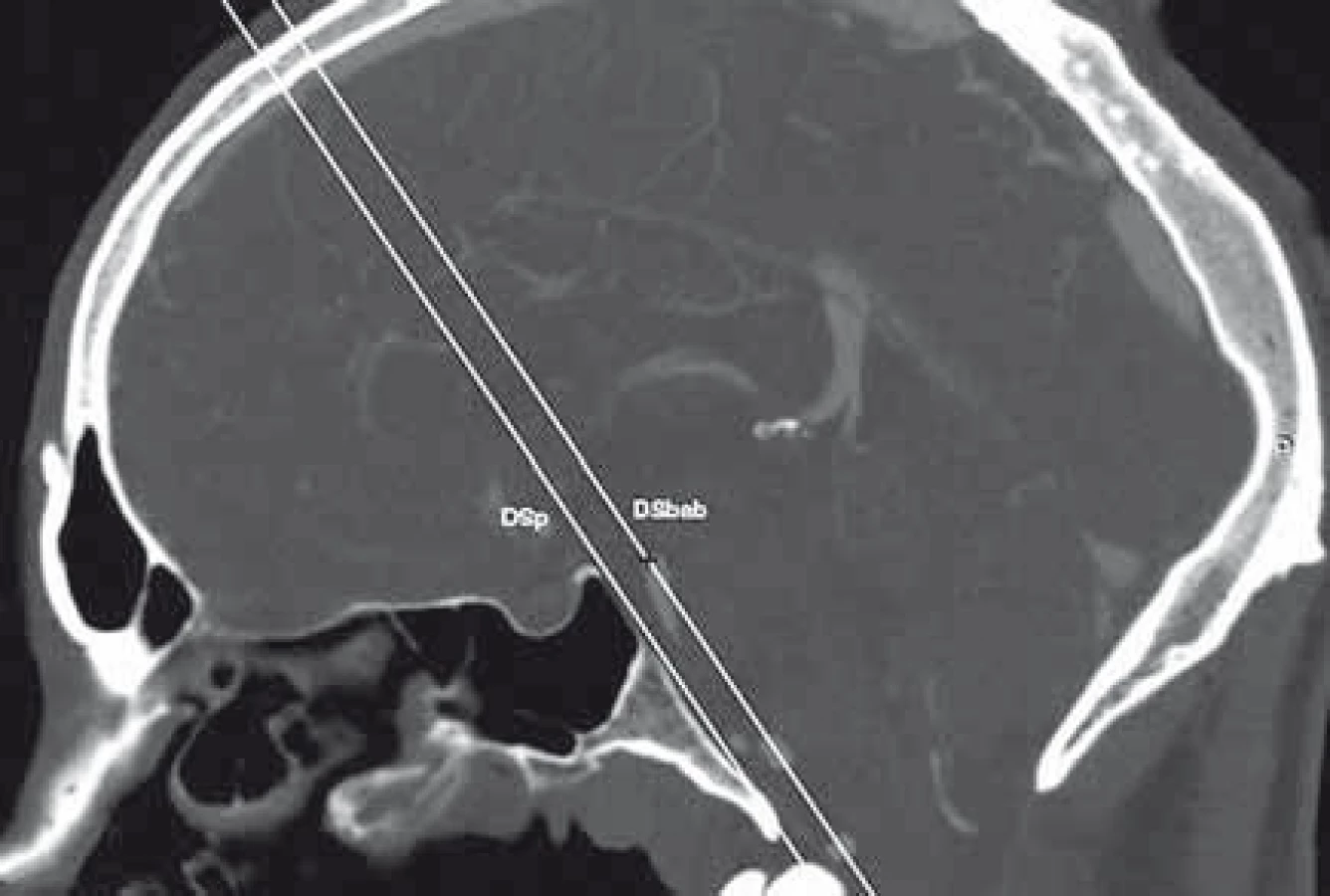
- C. In order to evaluate the distance between the BAB and the DS in the sagittal section, the following two planes were selected: the oblique coronal plane DSp in the Wackenheim clivus baseline and the oblique coronal plane DSbab parallel to the DS plane and encompassing the BAB (Fig. 4).
BAB – basilar artery bifurcation; BABsag – sagittal BAB; L – left; MP – middle plane; MP-BABsag – distance between the MP and BABsag expressed in mm; R – right
+ a marker
Obr. 2. Uložení BAB ve vztahu k MP. Koronární rekonstrukce CTA hlavy.
BAB – bifurkace bazilární arterie; BABsag – sagitální rovina BAB;
L – vlevo; MP – střední rovina; MP-BABsag – vzdálenost mezi MP
a BABsag vyjádřená v mm; R – vpravo
+ označení
BAB – basilar artery bifurcation; BABtp – transverse BAB plane; L – left; R – right; TP – transverse plane; TP-BABtp – distance between the TP and BABtp expressed in mm
+ a marker
Obr. 3. Uložení BAB ve vztahu k TP. Koronární rekonstrukce CTA hlavy.
BAB – bifurkace bazilární arterie; BABtp – transverzální rovina BAB; L – vlevo; R – vpravo; TP – transverzální rovina; TP-BABtp – vzdálenost mezi TP a BABtp vyjádřená v mm
+ označení
BAB – basilar artery bifurcation; DS – dorsum sellae; DSp – DS plane; DSp-DSbab – distance between the DS plane and DSbab expressed in mm, which represents the distance between the BAB and DS
+ a marker
Obr. 4. Vzdálenost mezi BAB a DS. Sagitální rekonstrukce CTA hlavy.
BAB – bifurkace bazilární arterie; DS – dorsum sellae; DSp – rovina DS; DSp-DSbab – vzdálenost mezi rovinami DSp a DSbab, vyjádřená v mm, která odpovídá vzdálenosti mezi BAB a DS
+ označení
Statistical analysis
Statistical calculations were performed in PQStat version 1.6.2.901 (PQStat Software, Poznań/ Plewiska, Poland).
The BAB symmetry in relation to the MP and TP in men and women was analysed using the chi2 test and Fisher’s exact test.
The position of the BAB depending on gender was compared using the Student’s t-test.
The position of the BAB depending on age was analysed with the Student’s t-test for independent samples.
The tested probability was deemed significant at p < 0.05, and highly significant at p < 0.01.
Results
BAB symmetry in relation to the MP and TP
In the studied patients (n = 100), the BAB was located on the right of the MP in 57% of the cases, on the left of the MP in 41% of the cases and medially in 2% of the cases.
The BAB was located above the TP in 47% of the cases and below it in 53% of the cases. There were no cases with the BAB located in the TP (Tab. 1).
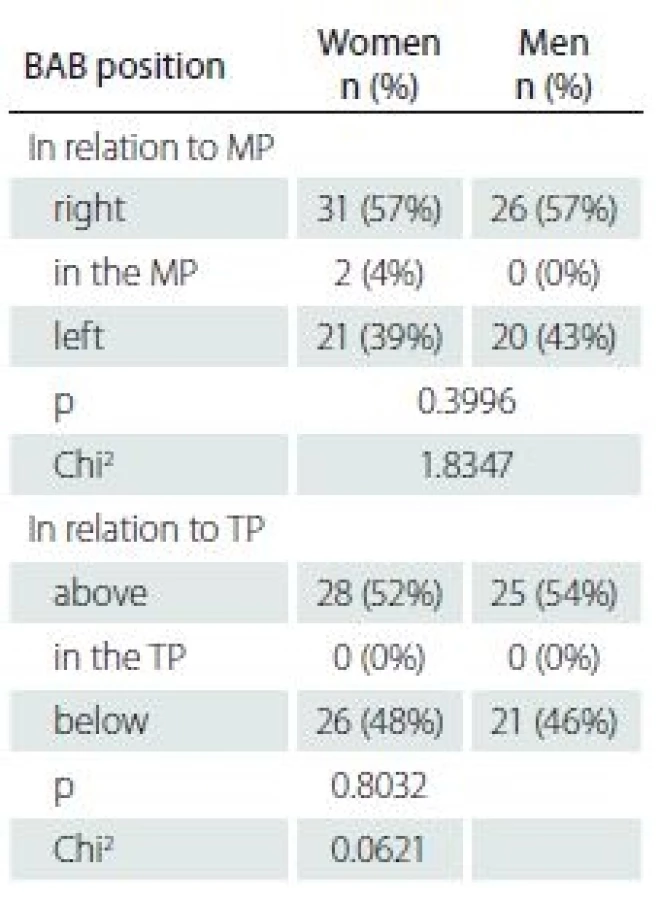
There were no significant differences (p > 0.05) between BAB symmetry and the investigated planes (MP and TP) depending on gender.
Position of the BAB in relation to the DS
In the studied patients (n = 100), the mean distance between the BAB and MP was – 0.35 mm (the BAB was located on the right of the MP), and the mean distance between the BAB and TP was – 1.01 mm (the BAB was located below the TP). The mean distance between the BAB and DS was 9.34 mm (Tab. 2).
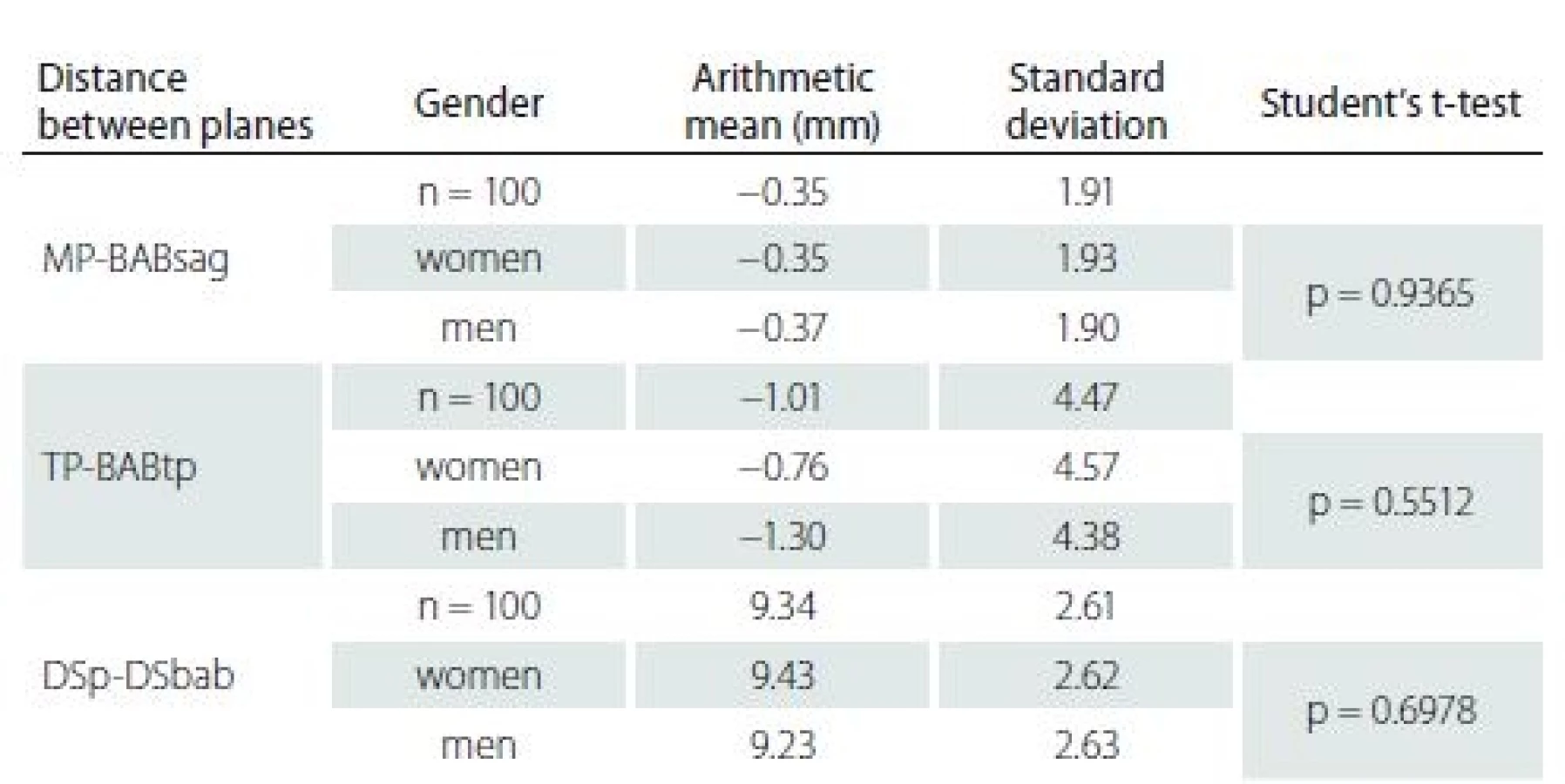
There were no significant differences (p >0.05) between BAB position depending on gender.
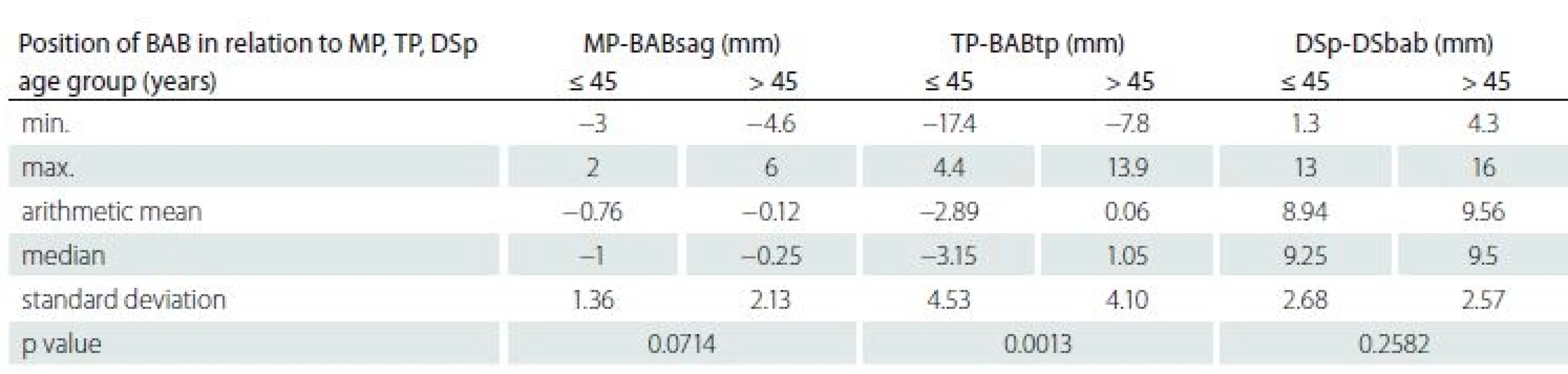
Position of the BAB depending on age
The position of the BAB in relation to the DS was also analysed in two groups of patients: group 1 – above 45 years of age and group 2 – up to 45 years of age. As for the BAB location in relation to the TP (in relation to the DS), the study revealed a statistically significant difference (p < 0.01) and higher BAB position in persons above 45 years of age (Tab. 3).
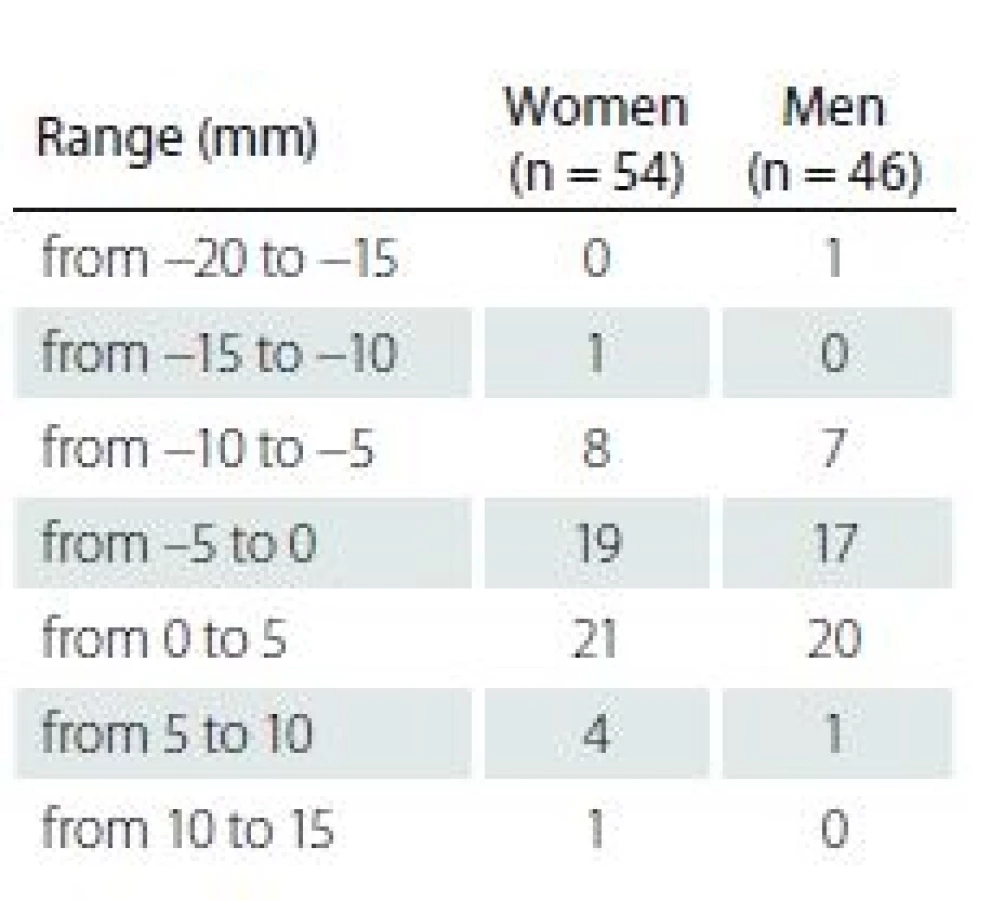
Position of the BAB in relation to the TP (height ranges)
The position of the BAB in relation to the TP was evaluated in seven 5-millimetre height ranges. In 41% of the cases, the BAB was found between 0 mm and 5 mm above the TP; this was the most common range. The location of the BAB in extreme ranges (from – 20 mm to – 15 mm and from 10 mm to 15 mm) was the rarest and noted in only 1% of the cases (Tab. 4).
The diagrams (Fig. 5 A, B) show the position of the terminal BAB (red spot) in women (n = 54) and men (n = 46) in a two-dimensional Cartesian coordinate system, where:
- point 0, called the origin of the coordinate system, was set at a point where the perpendicular axes x and y meet;
- x, the abscissa, represents the TP;
- y, the ordinate, represents the MP.
BAB – basilar artery bifurcation; MP – middle plane; TP – transverse plane
Obr. 5. Uložení BAB ve vztahu k ose x (TP) a y (MP) – A u žen (n = 54); B u mužů (n = 46) (škála od –20 do 20 mm).
BAB – bifurkace bazilární arterie; MP – střední rovina; TP – transverzální rovina
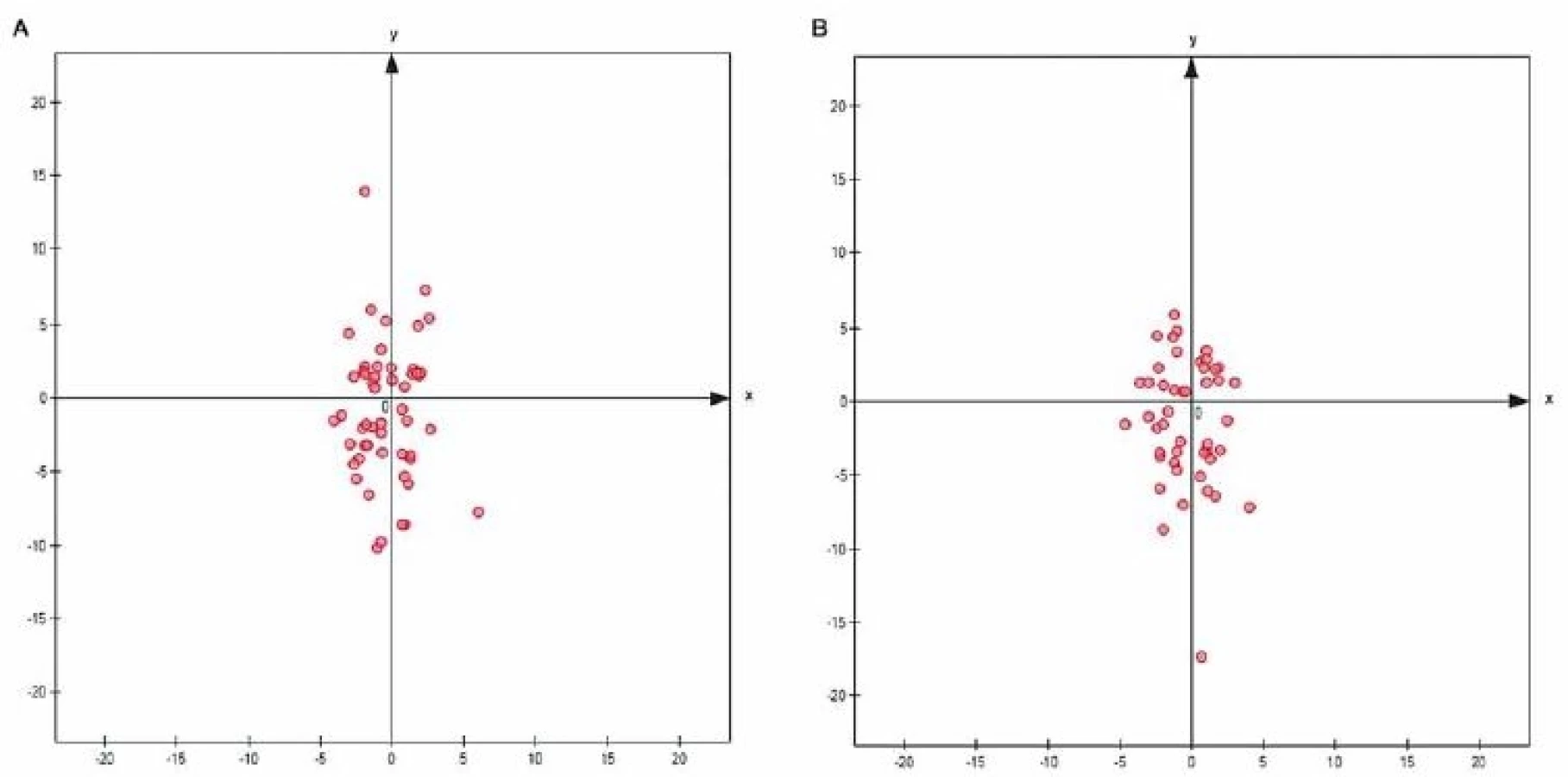
The following values were assumed to determine the BAB:
- negative values: position of the BAB on the right of the MP (y axis) and below the TP (x axis),
- positive values: position of the BAB on the left of the MP (y axis) and above the TP (x axis).
Discussion
Surgery for BAB aneurysms is essential when the method of choice, i.e. endovascular treatment, cannot be applied [14]. BAB aneurysm clipping is performed in a narrow and deep surgical field. Surgical difficulties result from the location of the BAB in the neighbourhood of vital anatomical structures, such as the brain stem, internal carotid artery, pituitary gland, oculomotor nerve or perforators that supply the diencephalon and mesencephalon [11].
According to Yamaura et al., the position of a BAB aneurysm in relation to the DS plays a significant role in surgical planning [16]. Tjahjadi et al., however, disagree. They believe that the height in relation to the posterior clinoid process should be the point of reference [3]. Moreover, Majchrzak et al. also indicate that the position of the BAB in relation to the line between the posterior clinoid processes is significant in the selection of a surgical approach to aneurysms in this region [17]. Caruso et al., in turn, claim that a surgical approach should depend on the distance of the BAB from the DS [18].
Smoker et al. have analysed the BAB position in relation to the DS in CT scans of the head (5-mm cuts) in 126 patients. The BAB was found at the level of the suprasellar cistern (one cut above the DS) in 71 patients (56%), whereas 45 patients (36%) had the BAB located at the level of the DS or below it. The least numerous group were 10 patients (7.9%) with the BAB found at the level of the floor of the third ventricle (one cut above the suprasellar cistern) [19].
In the present study, the analysis of 100 CTA scans (54 women and 46 men) showed that the mean distance of the BAB in relation to the TP was 1.01 mm below the TP, with most cases (41%) found in the range from 0 to 5 mm above the TP.
In the study by Żurada et al., the mean distance between the BAB and DS, evaluated in CTA head scans of 98 patients, was 9.55 mm [20]. In our study, the mean distance between the BAB and DS was 9.34 mm. Smoker et al., on the other hand (n = 126), found the BAB in the midline in 69 patients (55%), in the paramedian position (medial to the lateral margins of the DS) in 22 patients (17.4%) and in the medial right position in 33 patients (26%) [19].
The right location of the BAB in relation to the MP was found in our study in 57% of the cases with the mean distance from this plane at the level of 0.35 mm.
As did Żurada et al. [20], we did not find any significant differences in the BAB position in relation to the DS depending on gender. However, the statistical analysis of the results depending on age showed a highly significant difference (p < 0.01) and a higher BAB position above the TP (mean 0.06 mm) in patients above 45 years of age. This may reflect the tendency toward basilar artery elongation with age. Such a position limits the possibilities of Drake’s and pterional approaches. A different angle of view is offered by fronto-orbito-zygomatic approaches, where the trajectory runs upwards from below without significant retraction of the temporal lobe.
Gonzalez et al. have divided aneurysms found in this region depending on the position in relation to the DS. They distinguished: high-lying lesions for aneurysms located 5 mm above the DS and low-lying lesions for aneurysms located 5 mm below the DS [21]. In our study, the position of the BAB in relation to the DS was evaluated in 5-mm ranges. In most cases (41%), the BAB was found between 0 mm and 5 mm above the DS.
Conclusions
This study proposed methodology to facilitate accurate and reproducible determination of the BAB distance from the DS. The authors believe that it may help plan safe surgical approaches to basilar tip aneurysms, particularly in patients with the BAB located near the DS.
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
The Editorial Board declares that the manuscript met the ICMJE “uniform requirements” for biomedical papers.
Wojciech Ilków
Department of Neurosurgery
University Teaching Hospital in Opole
al. Witosa 26
45-401 Opole
Poland
e-mail: wojciechilkow@gmail.com
Accepted for review: 1. 2. 2018
Accepted for print: 18. 7. 2018
Zdroje
1. Rhoton AL Jr. Anatomy of saccular aneurysms. Surg Neurol 1980; 14(1): 59– 66.
2. Michalik R, Ciszek B, Ząbek M et al. Anatomy of distal division of the basilar artery. Przegl Lek 1996; 53 (Suppl 1): 107– 110.
3. Tjahjadi M, Kivelev J, Serrone JC et al. Factors determining surgical approaches to basilar bifurcation aneurysms and its surgical outcomes. Neurosurgery 2016; 78(2): 181– 191. doi: 10.1227/ NEU.0000000000001021.
4. Jamieson GK. Aneurysms of the vertebrobasilar system; surgical intervention in 19 cases. J Neurosurg 1964; 21: 781– 797. doi: 10.3171/ jns.1964.21.9.0781.
5. Drake CG. Surgical treatment of ruptured aneurysms of the basilar artery. Experience with 14 cases. J Neurosurg 1965; 23(5): 457– 473. doi: 10.3171/ jns.1965.23.5.0457.
6. Marchel A, Bidziński J, Bojarski P. Clinical analysis and the results of surgical treatment of aneurysms of the vertebrobasilar system. Neurol Neurochir Pol 1992; 26(2): 192– 200.
7. Majchrzak H, Kopera M. Basilar bifurcation aneurysms. Przegl Lek 1996; 53 (Suppl 1): 71– 74.
8. Lawton MT. Basilar apex aneurysms: surgical results and perspectives from an initial experience. Neurosurgery 2002; 50 (1): 1– 8. doi: 10.1097/ 00006123-200201000-00002.
9. Eskridge JM, Song JK. Endovascular embolization of 150 basilar tip aneurysms with Guglielmi detachable coils: results of the Food and Drug Administration multicenter clinical trial. J Neurosurg 1998; 89(1): 81– 86. doi: 10.3171/ jns.1998.89.1.0081.
10. van Rooij WJ, Sluzewski M. Procedural morbidity and mortality of elective coil treatment of unruptured intracranial aneurysms. AJNR Am J Neuroradiol 2006; 27(8): 1678– 1680.
11. Sugita K, Kobayashi S, Takemae T et al. Aneurysms of the basilar artery trunk. J Neurosurg 1987; 66(4): 500– 505. doi: 10.3171/ jns.1987.66.4.0500.
12. Chanda A, Nanda A. Anatomical study of the orbitozygomatic transsellar– transcavernous– transclinoidal approach to the basilar artery bifurcation. J Neurosurg 2002; 97(1): 151– 160. doi: 10.3171/ jns.2002.97.1.0151.
13. Hernesniemi J, Ishii K, Niemelä M et al. Subtemporal approach to basilar bifurcation aneurysms: advanced technique and clinical experience. Acta Neurochir Suppl 2005; 94: 31– 38. doi: 10.1007/ 3-211-27911-3_6.
14. Chalouhi N, Jabbour P, Gonzalez LF et al. Safety and efficacy of endovascular treatment of basilar tip aneurysms by coiling with and without stent assistance: a review of 235 cases. Neurosurgery 2012; 71(4): 785– 794. doi: 10.1227/ NEU.0b013e318265a416.
15. Drake CG. Treatment of aneurysms of the posterior cranial fossa. In: Krayenbühl H, Maspes PE, Sweet WH (eds). Microsurgical approach to cerebro-spinal lesions. Basel: Karger 1978: 122– 194.
16. Yamaura A, Ise H, Makino H. Treatment of aneurysms arising from the terminal portion of the basilar artery – with special reference to the radiometric study and accessibility of trans-sylvian approach. Neurol Med Chir (Tokyo) 1982; 22(7): 521– 532. doi: 10.2176/ nmc.22.521.
17. Majchrzak H, Ładziński P, Kopera M et al. Approaches to posterior circulation aneurysms and results of the operations. Neurol Neurochir Pol 2000; 34 (Suppl 6): 27– 34.
18. Caruso G, Vincentelli F, Giudicelli G et al. Perforating branches of the basilar bifurcation. J Neurosurg 1990; 73(2): 259– 265. doi: 10.3171/ jns.1990.73.2.0259.
19. Smoker WR, Price MJ, Keyes WD et al. High-resolution computed tomography of the basilar artery: 1. Normal size and position. AJNR Am J Neuroradiol 1986; 7(1): 55– 60.
20. Żurada A, St Gielecki J, Baron J et al. Interactive 3D stereoscopic digital-image analysis of the basilar artery bifurcation. Clin Anat 2008; 21(2): 127– 137. doi: 10.1002/ca.20598.
21. Gonzalez LF, Amin-Hanjani S, Bambakidis NC et al. Skull base approaches to the basilar artery. Neurosurg Focus 2005; 19(2): E3.
Štítky
Dětská neurologie Neurochirurgie NeurologieČlánek vyšel v časopise
Česká a slovenská neurologie a neurochirurgie

2018 Číslo 5
Nejčtenější v tomto čísle
- New insights in the diagnosis and treatment of amyotrophic lateral sclerosis
- Review of diseases with restricted diffusion on magnetic resonance imaging of the brain
- Cervical vertigo – fiction or reality?
- Anaesthesia and neuromuscular disorders