
Nové možnosti ultrazvuku v predikci výskytu bolesti dolní části zad u dospívajících mužů – pilotní studie
New possibilities of ultrasound in predicting low back pain in adolescent males – pilot study
Aim:
To determine the possible relationship between low back pain (LBP) and asymmetry of the cross-sectional area of the multifidus spinal muscle as measured by US in physically active and inactive adolescent boys.
Materials and methods:
In total, 45 adolescent boys were examined – 28 boys were physically active and 17 physically inactive. Height, weight, occurrence of back pain were recorded, and the spinal multifidus cross-sectional area was measured by US. The results were listed as mean, standard deviation, and percentage change of results. The difference between two samples was deducted using a two-tailed Student t-test (the level of significance was p < 0.05).
Results:
The results showed that the multifidus muscle size was larger in the physically inactive group (4.86 ± 1.91 cm2) than the physically active group (4.06 ± 1.42 cm2). The non-significant asymmetry expressed as a percentage of the cross-sectional area of the multifidus spinal muscle was found between boys who were physically active and physically inactive with back pain: 17.7 (14.1–21.0)% and 10.9 (3.3–18.5)%, resp.; and also without back pain: 6.9 (6.6–7.4)% and 7.5 (6.9–8.0)%, resp.; but the significant asymmetry expressed as a percentage of the cross-sectional area of the multifidus spinal muscle was found between boys with back pain and boys without back pain in both the physically active (p < 0.05) and physically (p < 0.05) inactive groups.
Conclusion:
The pilot study showed that there might be a relationship between back pain and asymmetry of the cross-sectional area of the multifidus spinal muscle. Further studies are needed to confirm these results.
Keywords:
adolescent – low back pain – multifidus muscle
超声预测青少年男性腰痛的新可能性 - 试点研究
目标:
通过超声(US)测量身体活动和非活动青少年男孩的腰背痛(LBP)和多裂肌脊柱横截面积的不对称性之间的可能关系。
材料和方法:
共检查了45名青少年男孩 - 其中28名男孩身体活动,17名身体不活动。记录身高,体重和背痛的发生,并通过US测量脊柱多裂肌横截面积。结果列为平均值,标准偏差和结果的百分比变化。使用双尾学生t检验推断两个样品之间的差异(显着性水平p <0.05)。
结果:
结果显示,物理非活动组(4.86±1.91 cm2)的多裂肌大小比物理活动组(4.06±1.42 cm2)大。非显着性不对称表现为多裂肌脊柱肌横截面积的百分比,发现身体活动和身体不活动的男孩与背痛:17.7(14.1-21.0)%和10.9(3.3-18.5)%分别;并且没有背痛:分别为6.9(6.6-7.4)%和7.5(6.9-8.0)%;但在身体活动(p <0.05)和身体(p <0.05)非活动组中,发现背痛的男孩和没有背痛的男孩之间的多裂肌脊柱横截面积的显着不对称性表示为。
结论:
初步研究表明,背部疼痛与多裂肌脊柱横截面积的不对称性之间可能存在关联。需要进一步的研究来证实这些结果。
关键词:
青春期 - 腰痛 - 多裂肌
Autoři:
R. Savickas 1; G. Krutulytė 1; D. Imbrasienė 2; V. Šiaučiūnaitė 3; I. Rimdeikienė 1
Působiště autorů:
Department of Rehabilitation, Medical Academy of Lithuanian University of Health Sciences Kauno klinikos, Kaunas, Lithuania
1; Lithuanian Sports University, Kaunas, Lithuania
2; Department of Mathematical Modelling, Kaunas University of Technology, Kaunas, Lithuania
3
Vyšlo v časopise:
Cesk Slov Neurol N 2019; 82(1): 96-99
Kategorie:
Krátké sdělení
doi:
https://doi.org/10.14735/amcsnn201996
Souhrn
Cíl:
Zjištění možné souvislosti mezi bolestí dolní části zad a asymetrií plochy průřezu páteřního musculus multifidus pomocí UZ měření u fyzicky aktivních a neaktivních dospívajících chlapců.
Soubor a metody:
Celkem bylo zkoumáno 45 dospívajících chlapců – 28 chlapců bylo fyzicky aktivních a 17 fyzicky neaktivních. Byly u nich zaznamenány výška, hmotnost, přítomnost bolesti zad a ultrazvukem byla změřena plocha průřezu páteřního musculus multifidus. Výsledky byly uvedeny jako střední hodnota, směrodatná odchylka a procentuální změna výsledků. Rozdíl mezi dvěma vzorky byl vypočítán pomocí dvouvýběrového Studentova t-testu (hladina významnosti činila p < 0,05).
Výsledky:
Z výsledků vyplývá, že velikost musculus multifidus byla větší ve skupině s fyzickou neaktivitou (4,86 ± 1,91 cm2) než ve skupině s fyzickou aktivitou (4,06 ± 1,42 cm2). Byla zjištěna nevýznamná asymetrie vyjádřená jako procento plochy průřezu páteřního musculus multifidus u fyzicky aktivních i fyzicky neaktivních chlapců s bolestí zad: 17,7 (14,1–21,0) %, resp. 10,9 (3,3–18,5) %, a také bez bolesti zad: 6,9 (6,6–7,4) %, resp. 7,5 (6,9–8,0) %, avšak významná asymetrie vyjádřená jako procento plochy průřezu páteřního musculus multifidus byla zjištěna mezi chlapci s bolestí zad i a chlapci bez bolesti zad jak ve skupině fyzicky aktivních (p < 0,05), tak ve skupině fyzicky neaktivních (p < 0,05).
Závěr:
Tato pilotní studie ukázala, že může existovat souvislost mezi bolestí zad a asymetrií plochy průřezu musculus multifidus. Pro potvrzení těchto výsledků jsou nutné další studie.
Klíčová slova:
dospívající – bolest dolní části zad – musculus multifidus
Autoři deklarují, že v souvislosti s předmětem studie nemají žádné komerční zájmy.
Redakční rada potvrzuje, že rukopis práce splnil ICMJE kritéria pro publikace zasílané do biomedicínských časopisů.
Introduction
Low back pain (LBP) is the leading cause of disability worldwide. It often begins in adolescence, setting a course for later in life. LBP is a relatively common complaint among children and adolescents [1,2]. It has been reported that the lifetime prevalence of LBP by age 20 is up to 80% [1]. Back pain is experienced at least once in a lifetime by 80−90% of adults. Back pain leads to lower working capacity, lower life quality, and costly pain medication. An increasing number of young adults and children turn to specialists for consultation on back pain. It has been established that from 15 to 25% of children suffer from recurrent or chronic back pain. Children complain about cranial, abdominal, and skeletal-muscular pain most frequently [1]. Various authors report different epidemiology of back pain in children. It varies from 17.6 to 26% among 11−17-year-old adolescents [2]. Among school students, it varies from 20 to 51% [3,4]. Other researchers have determined that 57.8% of school students experience back pain [5]. One-third (33.7%) of children and teenagers experience back pain at least once a week or more [1]. Quite a number (23%) of children turn to a physicist or a physiotherapist for consultation. A 25-year research project across schools in Denmark shows that back pain at the peak of growth is a risk factor for back pain at a later age [6]. Many studies have been conducted on children’s back pain and its causal factors. It has been proved that a link exists between back pain and physical activity. Mikkelsson et al. have studied the influence of flexibility, strength, and physical activity on the appearance of back pain in adolescents. The authors found that good flexibility in boys and good strength in girls had a link with cervical tension pain [6]. Other authors have linked back pain with low physical activity [7]. In other studies, authors have deducted that there is a link between back pain and a heavy school backpack, although other researchers say that a school backpack poses no influence on the appearance of back pain. Incorrect posture may be the cause of many complaints. Lithuanian and Polish studies on posture show that incorrect posture is abundant among children [8,9]. A significant relationship between back pain and psychosocial factors as well as children’s behaviour has been observed [3,10,11].
One of the causes of back pain is insufficient stability of the spine, which is dependent on the good function of surrounding muscles. A relationship has been found between the function of multifidus muscles, spinal stability and back pain [12]. Clinical testing has demonstrated that the cross-sectional area of the multifidus in people who experience back pain is about 10−30% smaller than in people who report no back pain [13]. All studies that have been conducted on deep back muscles were exclusively on adults. We failed to find any data on the multifidus muscles in children.
We hypothesise that the asymmetry in the multifidus muscle cross-sectional area is associated with back pain.
The aim was to determine the possible relationship between LBP and asymmetry of the cross-sectional area of the multifidus spinal muscle as measured by US in physically active and inactive adolescent boys.
Materials and methods
Study design
A cross-sectional design was used in a study conducted at one high school and one basketball school. The study was approved by the Bioethics Center (No. BEC-PT (M)-254). All of the participants provided their written informed consent prior to their inclusion in the study, in accordance with the ethical principles of the Declaration of Helsinki.
The study subjects were adolescent boys in the 7th grade of a high school and a basketball school. Written consent from each student’s parents or guardians was obtained. The study was performed before midday, before the children had the opportunity to become tired. The study data were recorded in anonymous questionnaires.
Participants
In a total of 45 boys, height, weight and the corss-sectional area of the multifidus muscle were measured and LBP was evaluated. The height of the boys in the target group was measured using a height measuring scale, and the weight was measured using an electronic weight scale. Pain was assessed using the McGill questionnaire [14] and a pain localisation map, which required specification of the localisation and description of the type of pain experienced. All the subjects received instructions on how to fill in the questionnaire.
Interventions
The cross-sectional area of the multifidus was measured using a TITAN US system, operating at the B-scan mode, 38- mm broadband linear array probe. The TITAN system is a portable, software-controlled US system using all-digital architecture. The ultrasonic muscle test is painless. It is non-invasive and does not use the ionising radiation method. The frequency of the measuring element was 7.5 MHz. The cross-sectional area of the multifidus was measured by a licensed US physician with 11 years of experience in measuring the multifidus muscle by US. The measurements were performed at the beginning of the study. The subjects were laid in the prone position with a symmetrical head posture, the chin resting against the examination couch, arms next to the sides of the trunk, and palms supine. The pairs of the spinal multifidus were measured at symmetrical locations. A tape measure and a marker were used to mark the points. The posterior superior iliac spines were chosen as starting points. The cross-sectional area of the multifidus was measured at both sides 3 cm above the posterior superior iliac spines, which is the equivalent of the level of the L4−L5 segments. Three images of multifidus muscle were taken and measured. The average of these three images were calculated and used for data analysis.
Statistical analysis
Statistical data analysis was performed using software packages Microsoft Office Excel 2007 (Microsoft Corporation, Redmond, WA, USA) and IBM SPSS Statistics Base 22.0 (IBM Corp., Chicago, IL, USA). The results of the study were processed using mathematical statistics methods for mean, standard deviation, and percentage change of results. The difference between two samples was deducted using a two-tailed Student t-test (the level of significance was p < 0.05).
The normality of distribution of the data was checked using Kolmogorov-Smirnov test, and not all parameters had normal distribution. To determine the reliability of abnormal distribution, we used the nonparametric Mann-Whitney U test.
Results
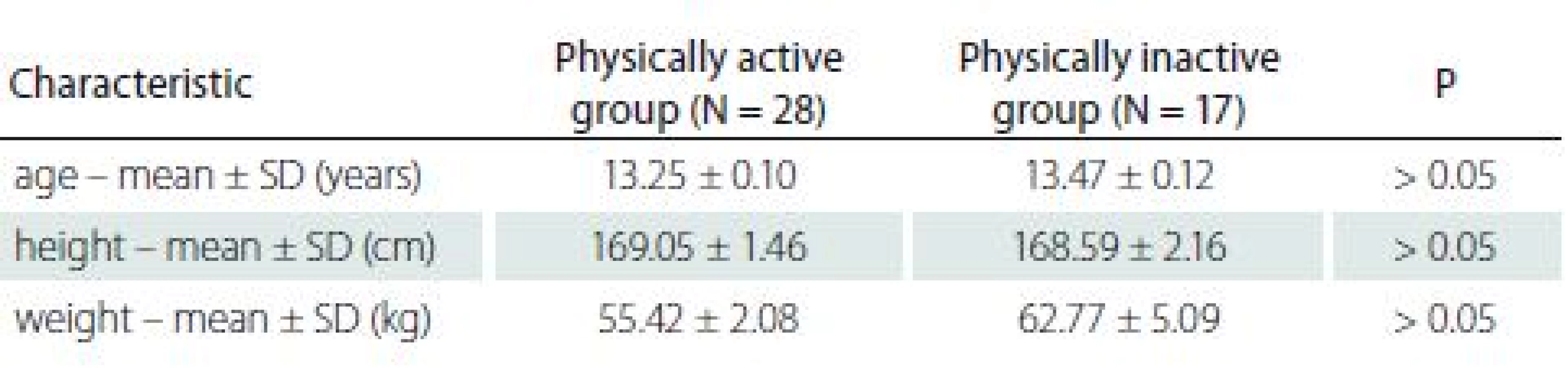
The adolescent boys were distributed into groups according to their physical activity: a group of physically active boys (N = 28) and a group of physically inactive boys (N = 17). The mean age of the subjects was 13.35 ± 0.06 years, the mean height was 168.9 ± 1.2 cm, and the mean weight was 58.2 ± 2.34 kg. Differences between groups were not statistically significant. The characteristics of all subjects’ means and standard deviations are demonstrated in Tab. 1.
The multifidus muscle cross-sectional area was measured by US. The results comparing the multifidus muscle size between healthy physically active and physically inactive boys and respectively those with LBP are demonstrated in Tab. 2.

*p = 0.023 by nonparametric Mann-Whitney U test
**p = 0.033 by nonparametric Mann-Whitney U test
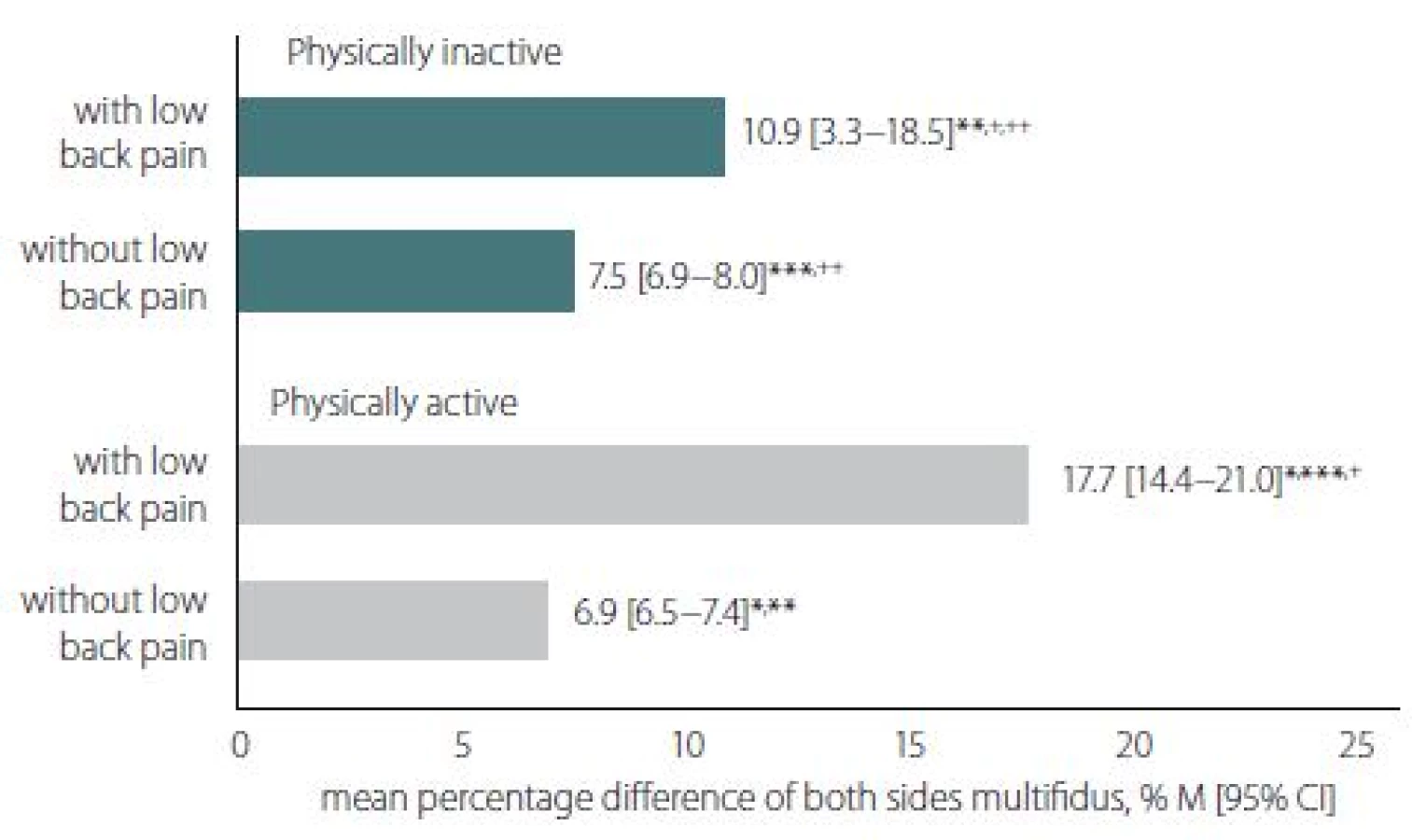
The non-significant asymmetry expressed as a percentage of the cross-sectional area of the multifidus spinal muscle was found between physically active boys and physically inactive boys with LBP: 17.7 (14.1–21.0)% and 10.9 (3.3–18.5)%, resp.; and also without LBP: 6.9 (6.6–7.4)% and 7.5 (6.9–8.0)%, resp. The significant asymmetry expressed as a percentage of the cross-sectional area of the multifidus spinal muscle was found between boys with LBP and boys without LBP in both physically active and physically inactive groups (Fig. 1).
* p = 0.001; **p = 0.014; ***p = 0.001
+ p = 0.036; ++p = 0.043
Discussion
The cross-sectional area of a muscle is directly related to its ability to produce force [13]. The asymmetry in multifidus muscles seems to promote LBP. Richardson et al. have performed studies of the cross-sectional area of the multifidus using US, where the cross-sectional area of the multifidus at the L2−L5 level was determined in 26 patients with acute LBP and in 51 healthy adults. The study showed that the affected segment muscle cross-sectional area was 8−31% smaller than in healthy adults. The muscle cross-sectional area asymmetry in healthy adults was only < 3−4% smaller. The function of the spinal multifidi was hindered by their decreased cross-sectional area: the damaged muscle was 10−30% smaller than healthy muscles [15].
Hides et al. stated that the patients with LBP had between-side differences in multifidus cross-sectional area of (mean ± standard deviation) 31 ± 8%; whereas the difference in the healthy controls was only 3 ± 4% [16]. The association between back pain and physical activity is proved. Mikkelsson et al. studied the influence of flexibility, endurance strength, and physical activity on the occurrence of back pain. Their study showed that good flexibility in boys and good strength endurance in girls could influence cervical tension pain [6]. Other authors have suggested that back pain had an association with low levels of physical activity [7]. We failed to find any studies reporting on the relationship between back pain and the cross-sectional area of the multifidus in adolescent males. We did not find a significant correlation between height and the cross-sectional area of the multifidus muscle or weight and the cross-sectional area of the multifidus muscle in adolescents. Little is known about the relationship between an adolescent’s weight and the cross-sectional area of the multifidus muscle. We also did not find any research on the cross-sectional area of the multifidus muscle in adolescents. This could be the objective of future studies. The study results showed that height and weight might have influence on the cross-sectional area of the multifidus muscle. We could assume that boys with asymmetry in the multifidus muscle cross-sectional area have back pain, regardless of their physical activity. Our hypothesis that the asymmetry in the multifidus muscle cross-sectional area may be the reason for the back pain is proved.
Limitations and recommendations
The main limitation of this study was the small sample groups. We have had difficulties interpreting the results, in particular confidence intervals and p-values. However, future similar studies with a larger sample size, in a wide age range group and also in both gender populations are recommended. It is also suggested that further studies can be designed to investigate the effect of stabilisation exercises on muscle size in the adolescent population and to follow the effect of the treatment programme in this age group.
Clinical applications
With support from further large-scale studies, the results of the present study seem to be helpful for clinicians and coaches to identify adolescents with LBP and then design the special treatment and training programme with special exercises for spine muscles.
Conclusion
The pilot study showed that there might be a relationship between back pain and asymmetry of the cross-sectional area of the multifidus spinal muscle. Further studies are needed to confirm these results.
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
The Editorial Board declares that the manuscript met the ICMJE “uniform requirements” for biomedical papers.
Raimondas Savickas, PhD, MD
Department of Rehabilitation
Medical Academy of Lithuanian University of Health Sciences Kauno klinikos
Eivenių 2
LT-50161 Kaunas
Lithuania
e-mail: raimondas.savickas@kaunoklinikos.lt
Accepted for review: 20. 4. 2018
Accepted for print: 10. 12. 2018
Zdroje
1. Roth-Isigkeit A, Thyen U, Stöven H et al. Pain among children and adolescents: restrictions in daily living and triggering factors. Pediatrics 2005; 115(2): 152–162. doi: 10.1542/ peds.2004-0682.
2. Jones GT, Macfarlane GJ. Epidemiology of low back pain in children and adolescents. Arch Dis Child 2005; 90(3): 312–316. doi: 10.1136/ adc.2004.056812.
3. Jones MA, Stratton G, Reilly T et al. Biological risk indicators for recurrent non-specific low back pain in adolescents. Br J Sports Med 2005; 39(3): 137–140.
4. Lafond D, Descarreaux M, Normand MC et al. Postural development in school children: a cross-sectional study. Chiropr Osteopat 2007; 15(1): 1–7. doi: 10.1186/ 1746-1340-5-1.
5. Shehab D, Al-Jarallah K, Al-Ghareeb F et al. Is low-back pain prevalent among Kuwaiti children and adolescents? A governorate-based study. Med Princ Pract 2004; 13(3): 142–146. doi: 10.1159/ 000076953.
6. Mikkelsson LO, Nupponen H, Kaprio J et al. Adolescent flexibility, endurance strength, and physical activity as predictors of adult tension neck, low back pain, and knee injury: a 25 year follow up study. Br J Sports Med 2006; 40(2): 107–113. doi: 10.1136/ bjsm.2004.017350.
7. Andersen BL, Wedderkopp N, Leboeuf-Yde C. Association between back pain and physical fitness in adolescents. Spine (Phila Pa) 2006; 31(15): 1740–1744. doi: 10.1097/ 01.brs.0000224186.68017.e0.
8. Boćkowski L, Sobaniec W, Kułak W et al. Low back pain in school-age children: risk factors, clinical features and diagnostic managment. Adv Med Sci 2007; 52 (Suppl 1): 221–223.
9. Krutulytė G, Valatkienė D, Samsonienė L et al. Evaluation of children age 11–12 posture according W. W. K. Hoeger visual method. Public Health 2007; 1(36): 16–20.
10. Hestbaek L, Leboeuf-Yde C, Kyvik KO. Are lifestyle-factors in adolescence predictors for adult low back pain? A cross-sectional and prospective study of young twins. BMC Musculoskelet Disord 2006; 7: 27. doi: 10.1186/ 1471-2474-7-27.
11. Steele E, Bialocerkowski A, Grimmer K. The postural effects of load carriage on young people – a systematic review. BMC Musculoskelet Disord 2003; 4: 12. doi: 10.1186/ 1471-2474-4-12.
12. Lee SW, Chan CK, Lam TS et al. Relationship between low back pain and lumbar multifidus size at different postures. Spine (Phila Pa) 2006; 31(19): 2258–2262. doi: 10.1097/ 01.brs.0000232807.76033.33.
13. Lieber RL. Skeletal muscle structure, function, and plasticity. 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins 2002.
14. Magee D. Orthopedic physical assessment. 5th ed. Edmonton: Saunders Elsevier 2008: 6–7.
15. Ranger TA, Cicuttini FM, Jensen TS et al. Are the size and composition of the paraspinal muscles associated with low back pain? A systematic review. Spine J 2017; 17(11): 1729–1748. doi: 10.1016/ j.spinee.2017.07.002.
16. Hides JA, Stokes MJ, Saide M et al. Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/ subacute low back pain. Spine (Phila Pa) 1994; 19(2): 165–172.
Štítky
Dětská neurologie Neurochirurgie NeurologieČlánek vyšel v časopise
Česká a slovenská neurologie a neurochirurgie

2019 Číslo 1
Nejčtenější v tomto čísle
- Lehká mozková poranění – konsenzuální odborné stanovisko České neurologické společnosti ČLS JEP
- Chronický subdurální hematom
- Oligoklonální IgG a volné lehké řetězce – srovnání izoelektrické fokusace v agarózovém a polyakrylamidovém gelu
- Ketogenní dieta – účinná nefarmakologická léčba dětské a adolescentní epilepsie